Why we use manual therapies with corrective exercises
Corrective exercises are used to correct abnormal function. However, in most cases the abnormal function is the central nervous system's... Read Article
Most websites will tell you that shoulder impingement is where tissues at the top of your shoulder get pinched, then give you a list of generic treatments such as exercises or therapies. Instead of these they should be asking why the pinching is happening in the first place. This is the reason shoulder impingement either doesn’t go away or keeps coming back: generic exercises and therapies are used instead of working out why the pinching actually occurs.
With that in mind so you can get your shoulder fixed properly, in this article I’ll use everyday language and easy to understand diagrams go over:
The key to properly fixing your shoulder impingement will be working out what has gone wrong and fixing that.
What is shoulder impingement
How your shoulder moves
What keeps your shoulder sitting and moving as it should
How these become abnormal: the real cause of shoulder impingement
Recommendations
References
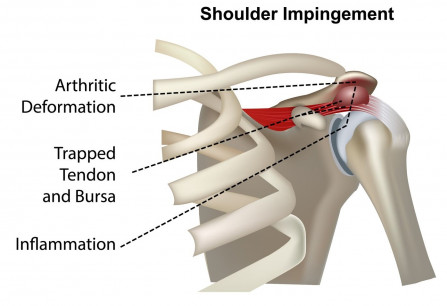
Most authoritative websites on shoulder impingement will have a diagram like this, showing that shoulder impingement is caused by tissues pinching in the small space at the top of your shoulder joint. To understand why it is pinching though we need to look at how your shoulder joint should move, what causes it to move normally, then what can go wrong with this.
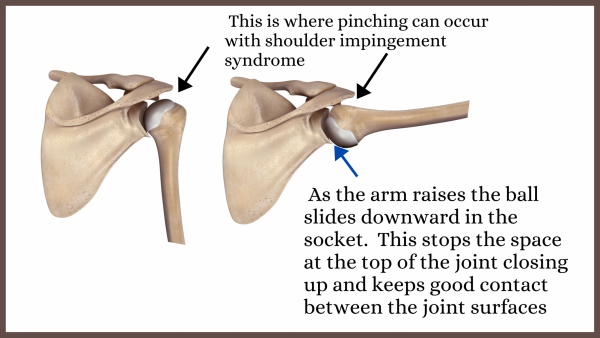
As this diagram shows your shoulder has a large ball sitting in a fairly shallow socket. It is designed like that to let your shoulder joint move a long way, but it is unstable so it needs a sophisticated control system to make sure the large ball stays sitting where it should be.
There are three things that work together to help keep the ball in your shoulder joint sitting and moving as it should.
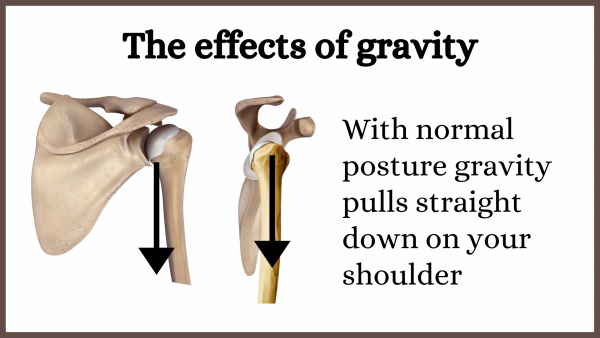
As this diagram shows, with normal posture the weight of the arm pulls straight downward on the ball of the shoulder joint.
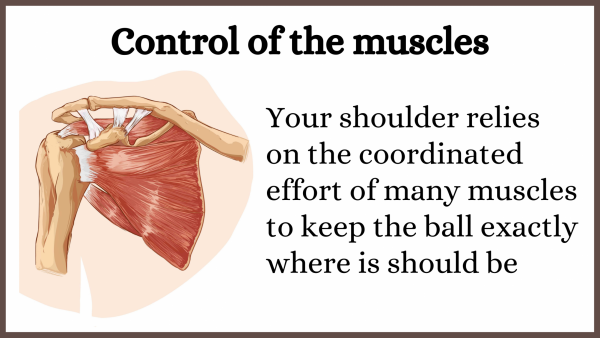
Muscles provide the main control of your shoulder joint position and movement. When your arm is just hanging by your side the muscles help counteract the pull of gravity. When your shoulder moves your shoulder muscles must go through a well orchestrated and coordinated effort to move your arm and keep the ball sitting properly in the socket. As a simple example, when you raise your arm the muscles at the top will tighten while at the same time the ones at the bottom will gradually let go.
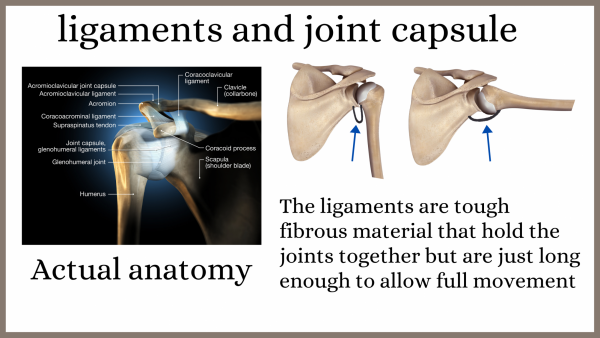
The capsule and ligaments are tough bands of tissue that hold joints together, allowing just enough slack for full movement. Under normal circumstances they don’t control the movement of the shoulder ball, just stop it moving too far. However, if something happens to change their length they can have an affect.
Here we'll look at how each of these can become abnormal, changing the way your shoulder joint moves and causing it to pinch.
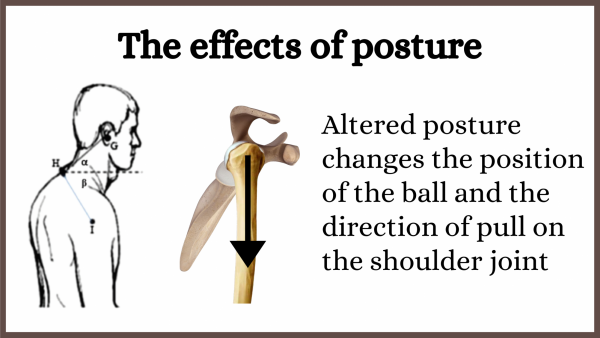
Scientists have found that one of the biggest causes of shoulder impingement is having a head and shoulders forward posture as shown in this diagram (1–7). This changes the position and pull of gravity on the ball in relation to your shoulder blade. The movement of your shoulder joint changes, plus the pull of gravity cannot be countered by the normal muscle pull. Over time this abnormal movement and stress will cause you to develop shoulder pain and maybe impingement.
An illustration of why generic fixes are so bad
At the start of this article I said that the main reason shoulder impingement wont go away or keeps coming back is that generic fixes are used and the cause of the pinching is usually not considered. Here is one of the main reasons why.
Although clinical trials and the laws of physics say that the head and shoulder forward posture will be a big problem for your shoulder medical journals usually ignore this. As an example, in it’s article Management of Shoulder Impingement Syndrome and Rotator Cuff Tears the journal American Family Physician makes no mention of this posture. Instead it gives generic treatment advice for doctors, which in summary is:
- start by modifying activities and taking anti-inflammatory drugs,
- do exercises to strengthen the shoulder muscles and increase the joint movement.
- If it’s still sore use injections, and if they they don’t work it’s off to the surgeon.
None of these therapies will do anything to change the abnormal posture that causes stresses and movement to be abnormal. Rest, drugs, injections and surgery will only mask the problem. The exercises could conceivably help the shoulder compensate, but with the mechanics of the shoulder joint being abnormal the movement and stress of the exercises will more likely cause further damage to the joint.
On the other hand correcting the posture would normalise the stress and movements of the shoulder, going a long way towards helping the problem resolve.
Now we’ve seen how gravity and posture can cause shoulder impingement lets look at muscles. As we’ve discussed muscles need to both hold the ball of the shoulder in position against gravity, and control it’s position when your arm moves.
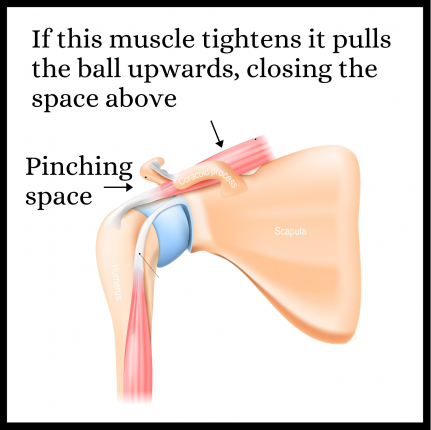
It’s simplest to look at the static (not moving) position of the ball first. It is held in position by gravity and the tension of the muscles. What that means is if one of the muscles is tight it will pull the ball in that direction.
As an example, the muscle attached at the top is called supraspinatus. Looking at the diagram of the shoulder, if supraspinatus tightens it will pull the ball upwards. This will closes off the space above, causing impingement.
It is the job of the muscles to keep the ball in the best position while the arm moves. In simple terms, if the ball needs to slide in one direction the muscle to that side will need to tighten while the muscle on the opposite side relaxes. The reality is that the actual movement needs the coordinates contraction (pulling) and relaxation of over a dozen muscles, but I hope you get the point. Anything that affects any of the individual muscles or affects the overall coordination of the muscles will cause the ball to move abnormally. At the minimum this will cause increased wear, long term arthritic changes and potential injury, and if the abnormal movement causes pinching you will get impingement syndrome.
With that, we'll look at the most common cause of abnormal muscle function: (myofascial) trigger points. For further information about these please see our article Trigger point basics. However, in summary they are those lumps in your muscles that therapists find. They cause muscles to:
Trigger points are the most common cause of the supraspinatus muscle being tight and cause pinching as discussed above. Treating the trigger point will often allow the muscle to relax, allowing the ball to drop so the pinching stops. As I discuss in our article Why do trigger points keep coming back trigger points need ongoing care to eliminate, but this is a great start.

Trigger points in the supraspinatus muscles are commonly caused by abnormal posture. This is an example where one problem (the posture) can cause a second problem (the trigger point) which then causes another problem (the change in joint function causing pinching). It is why fixing shoulder impingement (or any other muscluo-skeletal problem for that matter) needs detective work rather than “canned” generic therapies.
When muscles are unable to work normally your body needs to compensate. A Melbourne researcher Dr Karen Lucas did a trial where she wired up shoulder muscles with electrodes so her computer could monitor the activity of the many muscles while raising one's arm (8). She found that those people with no trigger points all had a nice smooth coordinated pattern of muscle activity, while those with trigger points in the shoulder muscles became un-coordinated. When Dr Lucas treated the trigger points and re-tested, the movement patterns had automatically returned to normal.

Exercises are commonly prescribed to correct these abnormalities. A couple of other research teams have have tried this and it doesn't work (9,10). The coordination of the muscles is abnormal because they are affected with trigger points. As Dr Lucas found, the way to restore normal muscle function is by treating trigger points.
Several teams of researchers have found that the muscles of shoulder pain sufferers are usually riddled with trigger points (11–15). This means that trigger point therapy needs to be performed before any corrective exercises are attempted.
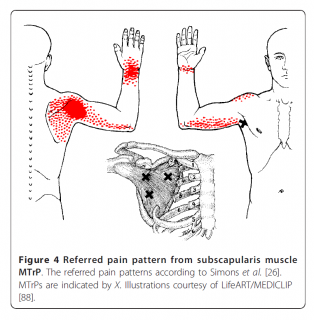
As well as potentially contributing to impingement trigger points also refer pain to your shoulder. A team of researchers found that treating trigger points in the shoulder muscles was excellent for relieving shoulder pain and improving shoulder function (16). This would have helped by both:
As we mentioned before, capsules and ligaments normally freely allow full movements, but nothing further. However there can be conditions or injuries that affect the length of these, possibly causing them to restrict movement, allow to much movement, or even pull on the ball altering it’s position. An experienced clinician should be able to identify this. They need to be corrected using specialised stretches or surgical techniques.
Something causing the ball to raise will reduce the space above the ball, but sometimes there will be something that reduces the space available. This may be an anatomical variant or arthritic changes thickening the surrounding bone.
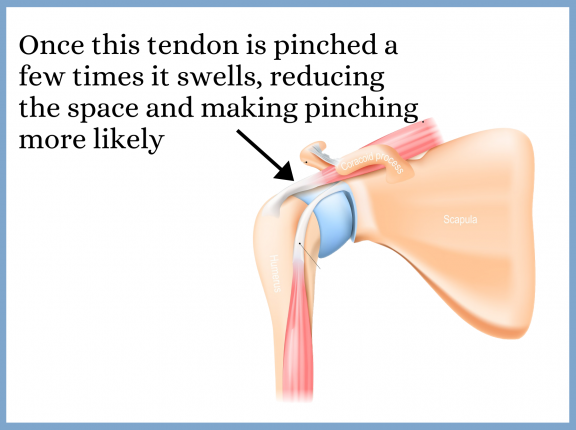
Alternatively the initial pinching may have caused the tendon that runs through this place to swell, occupying all of the space and leaving no gap around it. This is one time something like anti-inflammatory drugs or some sort of injection to temporarily reduce that swelling might be a good idea.
Thanks for reading this article. We’ve got an excellent article to help you get rid of the trigger point part of your problem. During my 27 plus years as a chiropractor I’ve hated seeing people whose shoulder problems had not got better and worsened over time time because they were given the typical inappropriate advice. If I can give you enough understanding to avoid that I am really happy. To get your shoulder fixed properly you’ll need a professional who works like a detective to solve the problems. If you sense that they get their info from the American Family Physician article I discussed or that you are being given some simple canned therapy go find another professional.
We are continually adding more information on research and uses. Subscribe below to have us email them to you "hot off the press".

Several years ago Dr Graeme, a Chiropractor practicing in Victoria, Australia was looking for a serious hand held massager his patients could use at home to get the extra quality massage they needed. The ones he found in the shops and on-line for home use looked nice but were not serious, and... read more
Corrective exercises are used to correct abnormal function. However, in most cases the abnormal function is the central nervous system's... Read Article
Please Wait, Processing Submission.
Do not refresh or leave this page until loading complete.